
INTRODUCTION
Ovarian cancer (OC) is a malignant neoplasm that ranks 18th in frequency of cancer and 14th in cancer deaths among women worldwide. In Mexico, it is the third leading cause of death from malignant tumors in women aged 30 to 59 years.
The risk factors associated with ovarian cancer (OC) are as follows: 1) Age, with the average onset between 60 and 65 years, of which 75% manifest after menopause; however, women who carry variants in the BRCA1/2 genes may develop the disease at an earlier age. 2) Genetics, where variants in these BRCA genes imply that the average cumulative risk of OC by age 70 is 59%, and involves association with cancer susceptibility syndromes, such as hereditary breast and ovarian cancer syndrome (HBOC), Lynch syndrome, Li-Fraumeni syndrome, among others. 3) A family history of OC and other associated neoplasms, such as breast and prostate cancer, increases the risk 3 to 4 times. 4) A history of previous cancer, for example, women who have had breast cancer with negative estrogen receptors and who have also been exposed to radiation have a 24% risk of developing OC compared to the general population. 5) Late menopause, defined as the occurrence of this event at age 55 or older, which is correlated with the total number of menstrual cycles experienced throughout a woman's life. 6) Nulliparity, which is associated with a 24% increase in risk compared to women who have given birth to at least one child, and this risk increases up to 12 times when compared to multiparous women. 7) Smoking, where active and regular smoking generates a risk of 85% to 125% in individuals who develop mucinous OC, compared to women who do not smoke. 8) Diets high in fats, especially common in North America and Western Europe, where there is a prevalence of the consumption of saturated animal fats and a lower intake of fiber. 9) Having undergone in vitro procedures, where an increased risk close to 20 times has been reported. Lastly, psychological stress is also recognized as a relevant risk factor for OC, as lifestyle changes promote high-risk behaviors, such as unbalanced diets, sedentary lifestyles, and substance use.
As for the symptoms of ovarian cancer, they can be vague at the onset of the disease, manifesting as colicky pain in the affected pelvic flank and/or abdominal distension, in addition to urinary urgency. In more advanced stages, symptoms may include difficulty breathing, secondary to the presence of ascites or pleural effusion, as well as the presence of a palpable tumor or one visible on ultrasound or tomography.
The histological classification of ovarian cancer (OC) according to its cellular lineage and degree of malignancy can be of three types: type 1 from epithelial cells, type 2 from germ cells, and type 3 from stromal cells. Type 1 OC from epithelial cells is the most common, occurring in approximately 90% of cases; its incidence increases with age, showing its peak during perimenopause. This, in turn, is divided into several epithelial subtypes, such as: high-grade serous with a frequency of 70-80%, endometrioid with a frequency of 10-20%, clear cell and low-grade serous, both with a frequency of 5-10%, mucinous at 3-5%, and carcinosarcoma at 1-3%.
High-grade serous carcinoma (HGSC), in addition to being recognized as the most prevalent and severe type, is also considered responsible for approximately 70 to 80% of the mortality associated with ovarian cancer; this is due to the presence of multiple genetic factors, such as the presence of variants that alter the protein function of TP53, which could occur in up to 96% or the presence of variants in BRCA genes, which can be observed in up to 20% of women with hereditary ovarian cancer. Identifying women with variants in the BRCA1 and BRCA2 genes impacts overall survival rates since there are specific treatments, such as PARP inhibitors (polynucleotide ADP-ribose polymerase), a synthetic therapy that eliminates cells with defects in double-strand DNA repair mechanisms caused by the presence of variants in these genes, thus contributing to the targeted elimination of cells.
According to Pietragalla A., et al., ovarian cancer could also be part of a hereditary cancer syndrome in 23% of cases, and due to its association with variants in BRCA genes (most of which produce a truncated protein), it may also be associated with other types of cancer such as pancreas, prostate, larynx, stomach, colon, and melanoma, among others [9]. Patients carrying a variant in the BRCA1 gene will have a 15-45% risk of developing ovarian cancer, while carriers of variants in BRCA2 will have a risk of 10 to 20%. However, 10-15% of patients with high-grade serous ovarian cancer will not present a deleterious variant, but rather will show variants of uncertain significance (VUS) that must be analyzed and reclassified, taking into account the family history and personal background of the patients [4, 11].
Due to its location, its rate of growth, its nonspecific symptoms, the few associated risk factors, and the lack of a screening test, the detection of ovarian cancer is generally in advanced clinical stages, and only 15% of cases will be confined to the ovary at the time of diagnosis; for this reason, it is considered one of the deadliest gynecological cancers and, consequently, a significant public health issue.
Identifying, diagnosing, and classifying patients with ovarian serous carcinoma (OSC) becomes a challenge for the Geneticist and Oncologist without the assistance of a genealogy or molecular study; since there are unique cases within the family that, due to the age of presentation, could guide us towards a hereditary cancer syndrome or actionable genes that could modify the comprehensive management of the patients. Therefore, the objective of this work is to describe from a genetic and molecular perspective, the characteristics of a sample of patients with high-grade serous ovarian carcinoma (HGSC), in order to support medical decision-making and promote a precise and effective approach for patients with this type of tumor.
MATERIALS AND METHODS
A prospective, observational, open, descriptive, and cross-sectional study was conducted during the period from 2017 to 2019, approved by the local committees. Mexican women referred from the Medical Oncology consultation, with a diagnosis of high-grade serous epithelial ovarian cancer (CO-SAG) confirmed by histopathological study, were included. The selected women were sent to the Oncogenetic consultation to be evaluated by an oncogeneticist; all the women signed the informed consent form after genetic counseling regarding the meaning of the possible result of the molecular study of the BRCA1 and BRCA2 genes. Subsequently, data of epidemiological and clinical interest were requested from each of them, which included place of residence, age, age at diagnosis, family history of cancers, clinical stage of the disease, among others.
A genealogy was performed for each of the women to investigate whether the CO could be part of a cancer susceptibility syndrome such as Hereditary Breast and Ovarian Cancer Syndrome (HBOC), Li-Fraumeni Syndrome, or Lynch Syndrome, according to the criteria established by the National Cancer Institute [12], or if it was a familial CO (family history with multiple types of cancer, without the presence of germline variants) or sporadic (without a family history of cancer).
The molecular study of the BRCA1 and BRCA2 genes was conducted in an external laboratory to our institution, using molecular analysis by next-generation sequencing (NGS) and/or by studying large rearrangements, in case there were no results from NGS. The results were received via email, and the patients were summoned to the oncogenetics consultation to complete the genetic counseling.
The epidemiological background of each patient was recorded in a database created in spreadsheet software to organize, analyze, and visualize the data for further analysis.
RESULTS
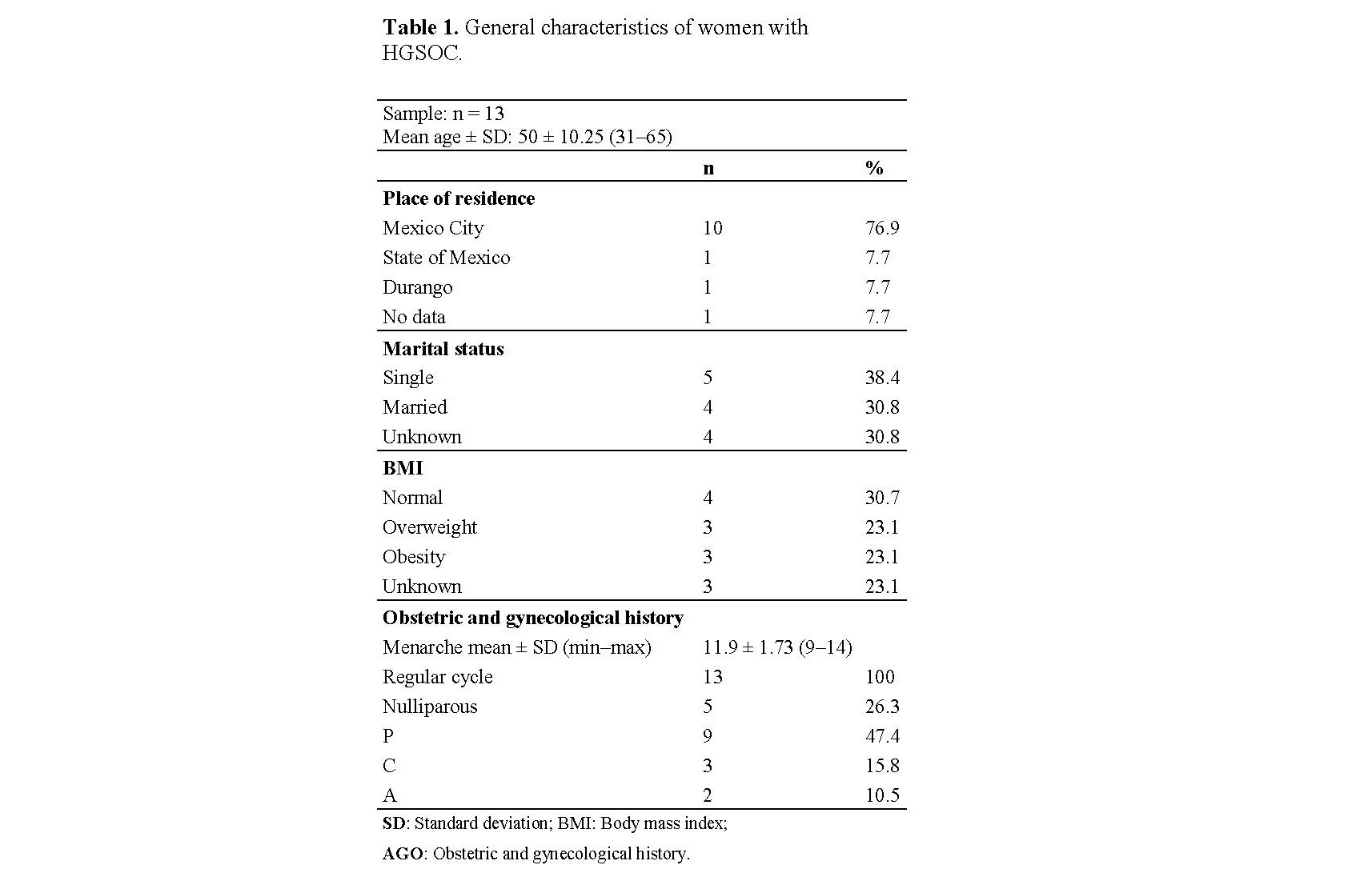
A total of 13 women of Mexican origin with a diagnosis of CO-SAG were included, with an average age of 50±10.25 years, of which 76.9% were residents of Mexico City and 38.4% were single. In the gynecological-obstetric history, it was observed that the average age of menarche in the women was 11.9 years; all women presented a regular rhythm. 26.3% had no pregnancies, while 47.4% had their children born by vaginal delivery, 15.8% by cesarean section, and 10.5% had an abortion (Table 1).
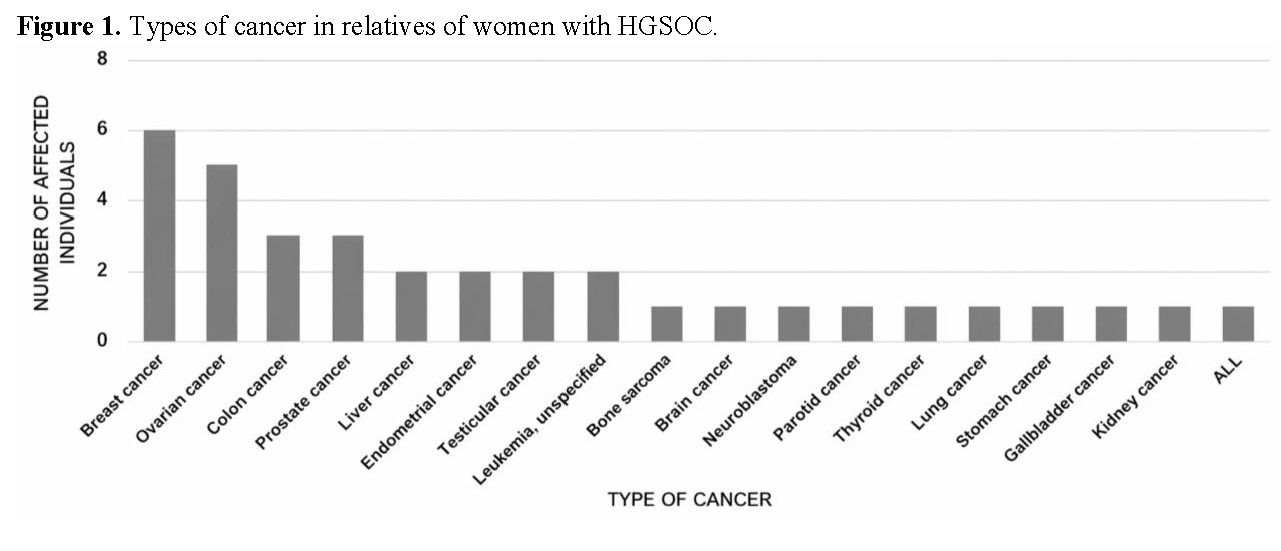
Regarding the hereditary family history of cancer (HFH), 92.3% (n=12) of the women had positive family histories, with the most frequently detected types of cancer being breast cancer (17.14%), followed by ovarian cancer (14.28%) and colon cancer (8.57%) (Figure 1).
The average age of diagnosis in the studied women was 47.85 ± 11.25 with a range of 31 - 65 years; when grouped by decades, we observed that more than 70% of them were diagnosed between the ages of 30 and 50 (Figure 2A). Furthermore, most women exhibited nonspecific symptoms associated with colitis or colicky abdominal pain, among the most frequent (Figure 2B).
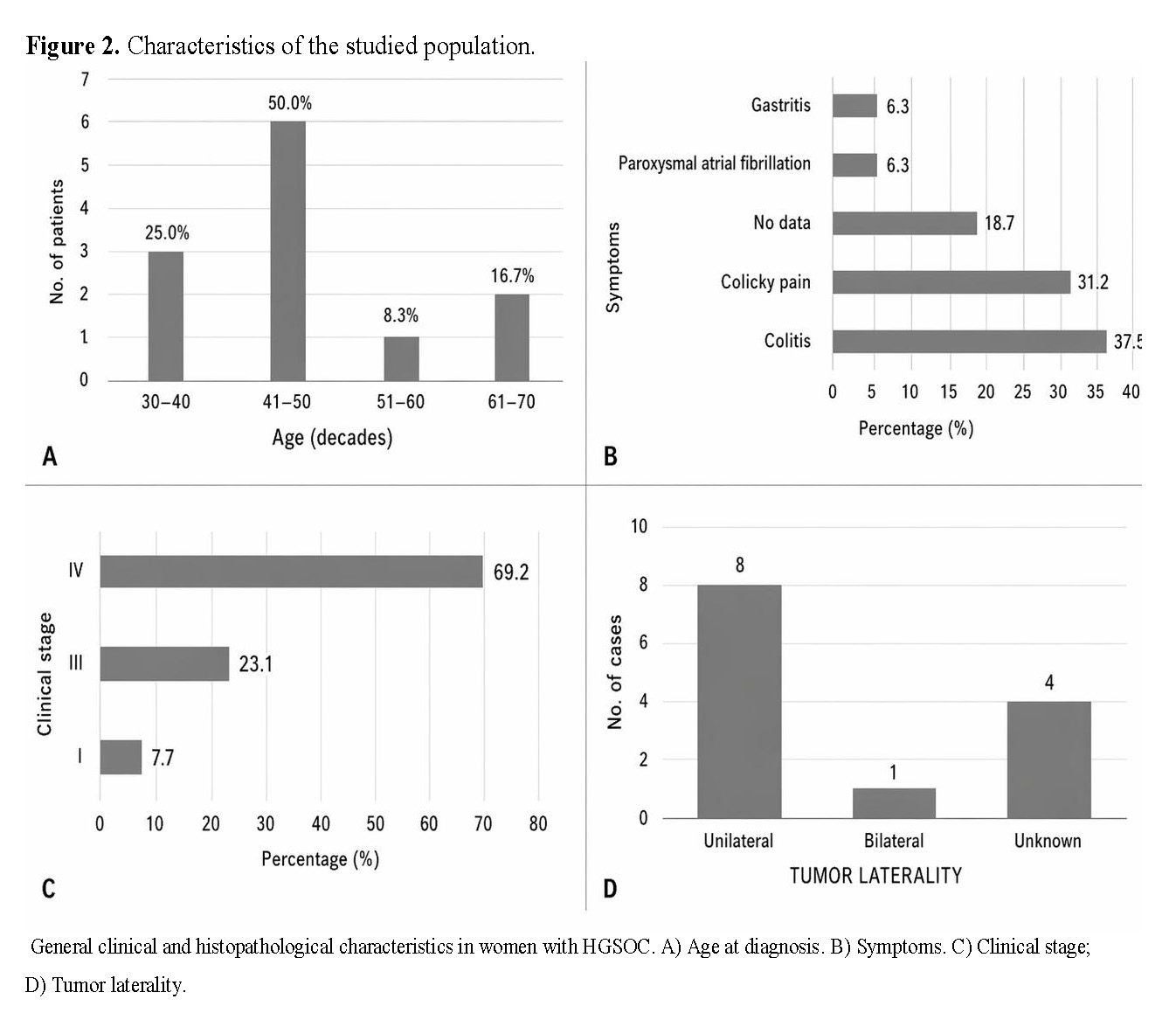
Regarding the staging of ovarian cancer, it was found that the predominant clinical stage in women with ovarian cancer was stage IV, in 69.2% of cases, followed by stage III and stage I, at 23.1% and 7.7%, respectively (See Figure 2C).
At the time of diagnosis, the predominant laterality of the ovarian tumor in the studied women was unilateral in 61.5% (n = 8), only 7.7% (n = 1) of the cases presented with bilateral tumor, and 30.8% (n = 4) had no data on tumor laterality in the records (Figure 2D).
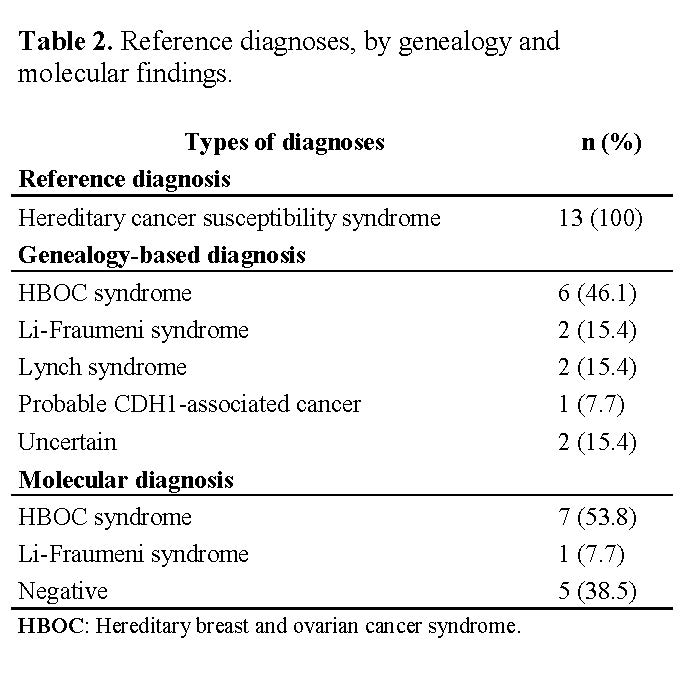
The diagnosis with which all the women were referred by the Oncology Service to the Oncogenetics service was probable hereditary cancer susceptibility syndrome; however, when genealogies were performed, they could be classified into 5 types of hereditary cancer syndromes, which included hereditary breast and ovarian cancer syndrome (HBOC), Li Fraumeni syndrome, Lynch syndrome, probable cancer associated with mutations in CDH1, and finally, the doubtful cases, those that, due to sharing several types of cancer between both parental lines, could not be classified into a specific type (Table 2).
Molecular studies of the BRCA1/2 genes showed that variants for the BRCA1 gene were found only in some cases, while no variants were found for the BRCA2 gene.
Table 3 shows the molecular characteristics of the BRCA1 gene at locus 17q21.31 found in 61.5% (n= 8) of the studied women with ovarian cancer, of which 15.4% (n= 2) had a deletion of exons 9-12, considered a pathogenic variant (PV) founder in the Mexican population; 7.7% (n= 1) had a deletion of exon 17 considered PV; 15.4% (n= 2) showed an intronic variant at the splice donor site and a non-conservative single nucleotide alteration that implies a reading frame change in exon 2, the first considered PV and the second probably pathogenic (VPP); and 23% (n=3) presented variants that produce a reading frame change involving a non-conservative single nucleotide alteration, considered PV. It is noteworthy that the 3 variants fall within the "ovarian cancer cluster region" (OCCR) in exon 11 of BRCA1, a region that in the SCMOH predominantly predisposes to manifest as ovarian cancer.
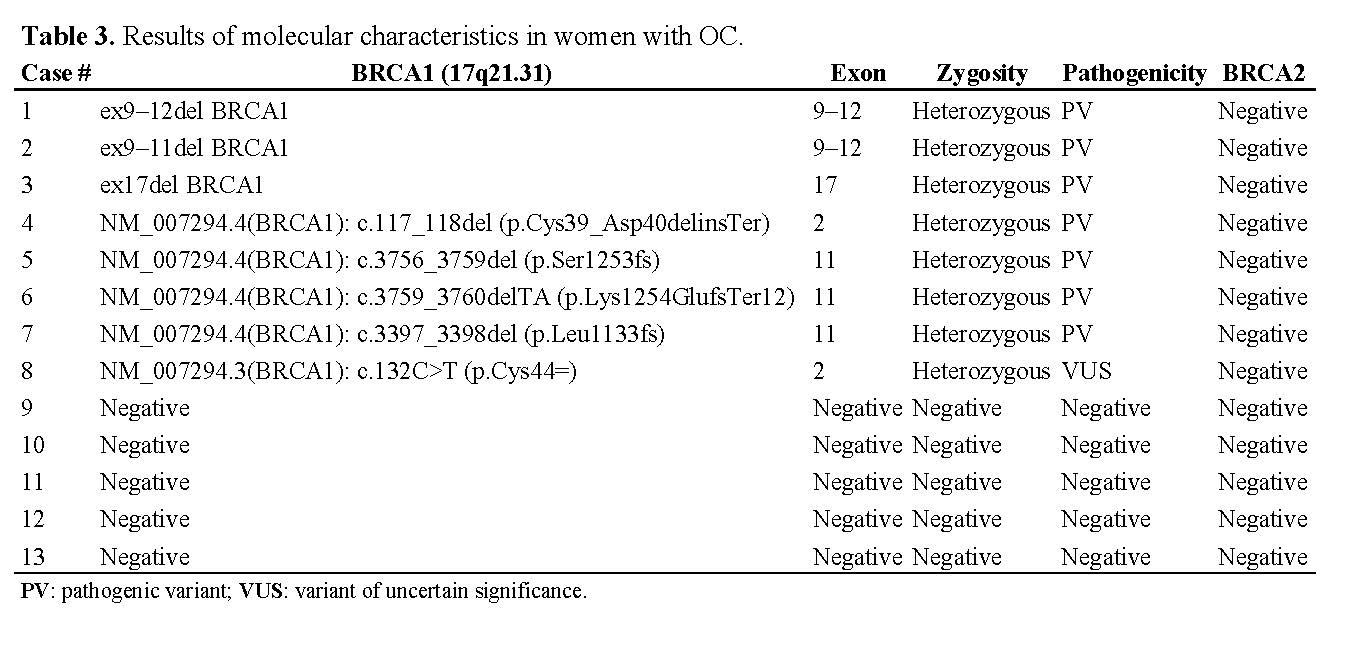
Regarding the representative genealogies for genetic counseling, we observed 3 specific cases. Case 7, which presents a VP, has no history of CO or other types of cancer in its genealogy and is also a young patient (38 years old). Case 8, with a VUS, shows a history of ovarian cancer and other related types of cancer in several generations in its genealogy. On the other hand, case 11 was negative for variants in both the BRCA1 and BRCA2 genes; however, it shows several relatives with CO and other types of cancer in its genealogy (Figure 3).

According to the National Comprehensive Cancer Network (NCCN) [13], if the BRCA gene results are negative, other prevalent genes associated with ovarian cancer should be considered, such as the TP53 gene of Li-Fraumeni Syndrome and the Mismatch Repair (MMR) system genes: MLH1, MSH2, MSH6, PMS2, or EPCAM of Lynch Syndrome as the second and third study options.
DISCUSSION
Epidemiological studies of CO show that by the year 2045, the increase in cases will be 40.4%, followed by a consequent increase in mortality of 53.2%. Furthermore, countries with low and middle-income, such as Mexico, will face a public health problem due to the lack of detection, surveillance, care, and novel treatment strategies for this pathology [14].
When addressing women with CO, family history, genealogy analysis, histopathological studies, and imaging studies help us make precise decisions for disease recognition and to provide counseling and monitoring for CO in women of reproductive and productive age.
Unfortunately, the diagnosis of the disease occurs at advanced clinical stages, because the symptoms of ovarian cancer are very nonspecific at the onset of the disease. This was demonstrated in this study where most women with ovarian cancer had at least one year prior, vague symptoms manifested as abdominal cramps or colitis and were diagnosed at an age between 30 to 50 years in advanced clinical stages III and IV.
For the above reasons, the detection of ovarian cancer (OC) through the two transcendent genes associated with the development of this type of cancer becomes imperative, since women carrying variants in the BRCA1/2 genes and their relatives have a permanent risk of OC of 39%-44% if they carry variants in BRCA1 and 11%-17% if they carry variants in BRCA2. Furthermore, these genes are important for risk recognition, predictive evaluation, and therapeutic approach in OC.
It is essential to highlight the importance of genetic counseling prior to conducting the molecular BRCA1/2 study, to determine if women with ovarian cancer wish to proceed with the study, as it is an autonomous and voluntary choice that involves the need to inform and support the patient about the possible risks, the type of inheritance in the family, and its medical implications, in order to make informed decisions based on data. Similarly, post-test genetic counseling serves to identify the primary cause, specifically analyze the results, and provide information related to prevention, management strategies, as well as possible treatments that may be available.
In this way, it is evidenced through genealogy and molecular results that a considerable number of women diagnosed with ovarian cancer have a family history of this type of cancer and other associated neoplasms, suggesting their inclusion in a cancer susceptibility syndrome. Among the most commonly identified syndromes are hereditary breast and ovarian cancer syndrome, Li-Fraumeni syndrome, and Lynch syndrome. However, in one of the analyzed cases (case 6), it is observed that having a family history of cancer is not essential to support the possibility of a cancer susceptibility syndrome and, therefore, the presence of a germline variant in BRCA1/2; the early onset of the disease could be the only indicator to consider the existence of a cancer susceptibility syndrome.
For women carrying variants in the BRCA1 genes, risk-reducing surgery such as bilateral salpingo-oophorectomy is recommended if they have fully completed motherhood and are between 35 and 40 years old, or in women between 45 and 50 years old classified within Lynch syndrome, as it reduces the risk of ovarian cancer by 81% during the 4 years following resection. However, there is the possibility of experiencing vasomotor symptoms, alterations in cardiac function, cognitive problems, osteoporosis, among others, if adequate preventive measures are not taken, due to the effects of premature surgical menopause.
Women in the early stages of ovarian cancer who wish to have children may opt for unilateral salpingo-oophorectomy, as the 5-year survival rates range from 100% to 66%, depending on the subtype of cancer and clinical stage, respectively.
It has also been described that young women carrying variants in BRCA genes who do not undergo bilateral salpingo-oophorectomy can be treated with oral contraceptives, which reduce the risk of ovarian cancer by 36% [1,13].
With the previously mentioned data, we have that for case 7 (Figure 3), genetic counseling consisted of informing the patient about a possible "de novo" mutation, as there is no other affected family member with cancer, as well as the risk of inheriting the variant. Therefore, extended studies for her family are suggested, since the variant is located in the OCCR and therapy with PARP inhibitors is recommended.
In case 8, which was initially classified as a VUS, it was informed during genetic counseling that it would be under monitoring, as over time the variant could modify its pathogenicity (as happened in this case), which went from VPP to VP.
Case 11 presents several relatives with colorectal cancer and other types of cancer; however, it shows a negative molecular study for variants in BRCA1/2. Genetic counseling is provided for a hereditary cancer susceptibility syndrome, and it is proposed to extend the molecular study for the patient and her relatives.
The established guidelines of the National Comprehensive Cancer Network (NCCN) recommend conducting genetic testing for other susceptibility genes for colorectal cancer when BRCA1/2 results are negative, such as TP53 in Li-Fraumeni syndrome, PTEN in Cowden syndrome, STK11 in Peutz-Jeghers syndrome, MLH1, MSH2, MSH6 in Lynch syndrome, as well as ATM, PALB2, RAD51C, and RAD51D, among others [1, 9, 13].
CONCLUSIONS
We present a case series of CO SAG in which the majority of cases showed familial histories and genealogies compatible with hereditary breast and ovarian cancer syndrome.
Histopathological and molecular studies are of great significance in patients with CO-SAG, as this histological type of cancer was associated, in this study, with 61.5% of cases to the BRCA1 gene.
Twenty-three percent (23%) of the women with hereditary breast and ovarian cancer (HBOC) had the variant located in exon 11 of BRCA1 in the region known as OCCR, a region that predisposes to a greater susceptibility to ovarian cancer. Meanwhile, 15.4% of the women with HBOC presented deletion of exons 9-12 of the BRCA1 gene, described as a founder mutation in the Mexican population for hereditary breast and ovarian cancer syndrome.
CONTRIBUTION
MOQ: Conceptualization, Data curation, Formal analysis, Methodology, Project management, Supervision, Validation, Writing (original draft), Writing (review and editing), LGO: Methodology, Validation, Writing (original draft), Writing (review and editing). GCS: Writing (original draft), Writing (review and editing).