
INTRODUCTION
Familial hemophagocytic lymphohistiocytosis (FHL), a type of hemophagocytic lymphohistiocytosis (HLH). This disease is a rare disorder of the autoimmune system presenting with an excessive inflammatory syndrome caused by activated T lymphocytes and histiocytosis, affecting almost all ages, with 70-80% presenting in the first year of life [1]. (Table1).
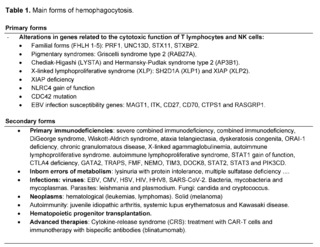
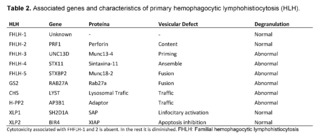
FHL can be divided into five subtypes according to the causative genetic variant. The pathogenic genes of FHL type 2 to 5 described are perforin 1 (PRF1), UNC-13 protein homologue D (UNC13D), syntaxin 11 (STX11) and syntaxin binding protein 2 (STXBP2), respectively; whereas, the genes for type 1 are still unknown [2] (Table 2). (See Table 1 and 2).
This disease presents with an autosomal X-linked recessive genetic variant that is commonly present in newborns or infants. Approximately 90% of children diagnosed are younger than 2 years and the incidence is approximately 0.12 per 100,000 [3]. Worldwide, 58% of patients with FHL have variants of the PRF1 gene, and as of 2018, 100 cases of familial hemophagocytic lymphohistiocytosis type 2 (FHL2) with identified PRF1 variants had been reported [4]. In Colombia, there is still no consolidated population burden. FHL is not part of the recognized orphan diseases [5]. In a 2021 national epidemiological bulletin on orphan diseases, it is described that 672 cases of blood diseases, hematopoietic organs and disorders affecting the mechanism of immunity were reported, 13.6% of the total, however, without discrimination of these [6].
NK cells and cytotoxic T lymphocytes (CTL) play an important role in the immune response to invading pathogens, predominantly viruses. They secrete soluble mediators such as interferon gamma (IFN-γ), which enhances immunity, interferes with viral replication and is also a potent macrophage activator. CTLs also mediate direct killing of infected cells and antigen presenting cells (APCs), including macrophages, predominantly through the release of cytotoxic granules [7]. During active disease there is a high serum concentration of IFN-γ, tumor necrosis factor alpha (TNF-α), interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10), interleukin 12 (IL-12), interleukin 18 (IL-18) and macrophage inflammatory protein 1 alpha (MIP-1α) [8].
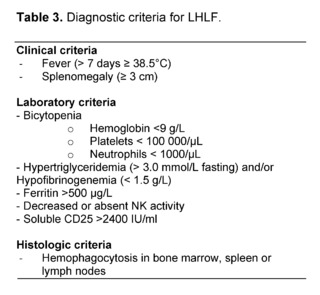
The main clinical features of this pathology are persistent fever, hepatosplenomegaly, pancytopenia, increased ferritin level, hypertriglyceridemia, hypofibrinogenemia, hepatitis and decreased NK cell activity [9,10], which can be detected in 20-73% of patients at initial clinical presentation. Patients with FHL may also present with neurological symptoms, such as seizures, facial paralysis, gait instability or even coma [11].The diagnosis should be made taking into account clinical, laboratory and histological criteria, and the diagnosis is established with 5 of the 8 (Table 3).
The main gene involved is PRF1, located in the 10q21.22 region containing three exons. The precursor of the encoded human perforin protein is mainly expressed in cytotoxic T lymphocytes and NK cells, which plays an important role in the regulation of the autoimmune system. Patients carrying defects in the PRF1 gene are vulnerable to infections, autoimmune diseases and malignancies [12]. Reduced production or activity level of perforin may result in impaired immune defense systems and dysregulation of apoptotic mechanisms. The hotspot variant in FHL2 is located in the conserved region 2 of protein kinase C. This domain is the key region for PRF1 protein to initiate membrane perforin and maintain cytotoxic activity. The altered PRF1 conformational change reduces the cytotoxic activity of the protein and causes disease [7].
The Histiocyte Society established a set of consensus diagnostic criteria that was revised in 2007 [10]. These criteria are useful to allow a clinical and laboratory diagnosis of FLH while more definitive molecular testing is being performed. Unless family history or genetic testing is consistent with FLH, patients should have five of the eight criteria. The HLH probability calculator (HScore) is another widely accepted diagnostic scoring system. The HScore is an online calculator that takes into account the following 9 criteria: the presence of immunosuppression, fever, visceromegaly, elevated triglyceride level, ferritin levels, serum aspartate aminotransferase/glutamic oxaloacetic transaminase levels, fibrinogen levels, presence of cytopenias, and hemophagocytosis in bone marrow samples. Each criterion is assigned a value based on logistic regression and a total score ranging from 0 to 337 is calculated from it. A higher score corresponds to a higher probability of HLH. The developers of the score found an optimal cutoff point of 169, which corresponded to a sensitivity of 93 % and a specificity of 86 % in their study [13]. The performance of the HScore was compared with the HLH-2004 criteria in adult and pediatric patients. The study concluded that the HScore is more predictive in the diagnosis of HLH than the HLH-2004 criteria. The sensitivity and specificity of the HScore were found to be higher in the pediatric group (100% and 80%, respectively) than in adults (90% and 79%, respectively) [14].
If FHL is suspected, paraclinicals should include complete blood count and blood smear, liver function tests, triglycerides, ferritin and coagulation profile. A bone marrow aspiration is performed and, if initially negative, should be repeated at a later stage if FHL is still a possible diagnosis. Lumbar puncture should be considered when there is suspicion of neurologic involvement. Rapid perforin detection can be performed by fluorescence-activated cell sorter (FACS) flow cytometry, which has allowed rapid identification of FHL2 [3]. FACS for perforin also identifies heterozygous FHL2 carriers. In addition, a granule release assay (GRA) has been developed that allows rapid detection of proteins involved in the transport and fusion of cytotoxic granules to the cell membrane, providing an alternative tool for the assessment of cytotoxic function of both T lymphocytes and NK cells [7]. The GRA assay is based on surface staining for the protein CD107a or also called LAMP1, which is present on the membrane of secretory granules within T cells and NK cells. Detection of CD107a on the cell surface after stimulation implies an intact pathway of granule exocytosis and normal function of the proteins in that pathway. The absence of CD107a expression on the cell surface suggests a defect in migration, docking, priming or fusion of secretory granules. However, assessment of NK cell degranulation is useful in identifying FHL type 3 to 5, but not FHL2, where granule exocytosis is normal [15].
Today, genomics is driving a fundamental shift in the diagnosis of rare diseases, from symptom analysis to molecular etiology assessment. Understanding the biological basis of disease can lead to better care and targeted treatment, with predictable evidence-based outcomes. This type of molecular diagnostics in rare disease genomics is the foundation of precision medicine. According to the American College of Genetics and Genomics (ACMG), identifying the genetic etiology of an individual's disease has utility for the patient, their family, and society at large [16]. An understanding of the mechanisms of rare diseases allows physicians to refer patients to appropriate specialists, select tailored therapeutics, and provide disease-specific follow-up. Similarly, defining the inheritance pattern of a rare disease informs recurrence risks for patients and both their immediate and extended families, supporting informed family planning.
Options for molecular genetic testing include the use of a multigene panel or genomic testing. A multigene panel can be used that includes analysis of genes involved in known types of FHL, such as PRF1, UNC13D, STX11, and UNC18B; however, a negative genetic study does not rule out HLH [17]. More than 90 variants in the PRF1 gene and more than 50 in the UNC13D gene have been identified in individuals with FHL [18].
In the past, various chemotherapeutic regimens targeting activated macrophages and histiocytes and T cells have been used as pharmacologic management. In 1994, the Histiocyte Society produced a consensus study protocol (HLH-94), which includes the combination of intravenous etoposide, oral or intravenous dexamethasone and, in patients with progressive neurological symptoms or abnormal cerebrospinal fluid, intrathecal methotrexate [1]. In recent decades, a modified protocol (HLH-2004) with the addition of oral cyclosporine was being used [10]. Initial treatment had a duration of 8 weeks, followed by maintenance therapy with etoposide at lower doses, prednisolone and cyclosporine A to maintain remission until HSCT was performed. A recent comprehensive study of HLH-94/2004 treatment regimens showed an overall response rate of 72.7% (complete response rate of 55.5%) and a 3-year overall survival rate of 74.7%, with an overall incidence of side effects of 18.2%. Although chemotherapy can temporarily alleviate symptoms, it cannot eliminate the genetic basis of immunodeficiency. As an adjunct, supportive treatment includes broad-spectrum antibiotics, prophylactic cotrimoxazole, oral antifungals, antiviral therapy if indicated, and intravenous immunoglobulin.
As for recent clinical trials, an interventional study was conducted in the United States, Canada, Germany, Italy, Spain, Sweden, Switzerland and the United Kingdom from 2019-2022, the purpose of which was to expand knowledge on the efficacy and safety of emapalumab as a treatment for patients with HLH, with special emphasis on long-term outcome and quality of life assessments. In October last year this study was completed, the investigators indicated that after completing treatment, patients will continue in the study for long-term follow-up up to 1 year after HSCT or the last emapalumab infusion (if HSCT is not performed), to make conclusions about the effectiveness of the drug [19]. Finally, a new study was initiated in early March 2023, which is not yet enrolling patients, aimed at studying patient survival until hematopoietic progenitor transplantation after the use of ruxolitinib as first-line treatment associated with corticosteroids in HLH [20].
CASE REPORT
Male patient, 11 years old, product of non consanguineous parents, with medical history of 6 episodes of recurrent pneumonia and 2 episodes of otitis before the age of 5 years, 1 episode of pansinusitis that required surgical procedure, eosinophilic esophagitis, gastroesophageal reflux disease, ulcerative colitis, asthma, suspected swallowing disorder, global developmental delay, dermatitis and chronic leukopenia. Mother and father with a history of pulmonary Mycobacterium tuberculosis and maternal grandfather with multidrug-resistant pulmonary Mycobacterium tuberculosis. The patient presented with de novo convulsive syndrome associated with intermittent fever, headache and emesis. Physical examination showed low weight and height for age, hepatomegaly, mild cognitive impairment and adaptive and school behavior below what was expected for his chronological age. Within the syndromic approach, hematologic, oncologic, immunologic, metabolic and infectious causes were ruled out.
Given the clinical complexity of the patient, given her family history, phenotypic heterogeneity, diverse clinical manifestations, possible differential diagnoses, inconclusive initial diagnostic tests and the suspicion of a complex genetic disease, a clinical exome for primary immunodeficiencies was requested, a diagnostic aid that analyzes exons of a set of known coding genes of the genome that could justify the present symptoms and confirm a specific pathology.
RESULTS
Whole exome sequencing was performed on a DNB-SEQ400 next-generation mass sequencer, in addition to copy number variants (CNV) by Next Generation Sequencing (NGS) for genes related to primary immunodeficiency (See supplementary files).
The sequencing results were analyzed bioinformatically in a secondary analysis (Leiden Open Variation Database (LOVD)) to evaluate the quality of the data obtained from sequencing and in a tertiary analysis to align the sequences, perform variant calling and filtering, meeting specific quality criteria. The identified variants were evaluated taking into account the parameters recommended by the ACMG guidelines for variant classification and their updates, including information from databases such as ClinVar, HGMD, LOVD, dbSNP and gnomAD.
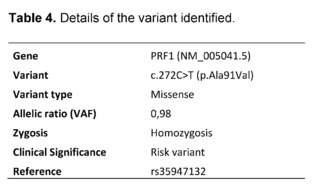
A homozygous A91V pathogenic variant was found in the PRF1 gene, this result could be related to FHL2 (Table 4). Pathogenic variants in the PRF1 gene (MIM *170280) are associated with autosomal recessive FHL2 (MIM #603553). A heterozygous variant has been identified in the PRF1 gene consisting in the substitution of a cytosine for a thymine at position 272 of the cDNA, in exon 2/3 of the gene (c.272C>T) and that at the protein level produces the missense change of an alanine for valine at codon 91 (p.Ala91Val), an amino acid residue located in the functional domain "PERF_HUMAN domain 'MACPF".
The described change has been reported in affected individuals with FHL2 in both heterozygosis and homozygosis (PMID: 17475905,32150605). Regarding the effect of this missense change in the gene or gene product, functional studies have been performed showing that the p.A91V variant results in protein misfolding and a secondary reduction in NK cell cytotoxicity, and it is proposed that this dysfunction in cytotoxicity is the cause of the immune-mediated disease in individuals as homozygous variants (PMID: 25776844). Patients with deleterious variants in the PRF1 gene have a higher risk or susceptibility than the general population to develop the conditions associated with the gene, especially considering the presence of the variant in homozygosis in a patient overlapping the phenotype described for the PRF1 gene, such as low weight and height, mild learning disability and pancytopenia; in addition to classic symptoms such as hepatosplenomegaly, fever and joint pain.
In this article, we report the case of a patient who, given the clinical complexity of his family history, phenotypic heterogeneity, diverse clinical manifestations, possible differential diagnoses, inconclusive initial diagnostic tests and the suspicion of a rare genetic disease, a targeted clinical exome was requested, where a homozygous pathogenic A91V variant was found in the PRF1 gene, a result related to FHL2.
The clinical picture and paraclinical findings were similar to those described in the literature. The PRF1 gene variant reported in this case was p.A91V, unlike that reported in a Chinese study where c.1349C>T is the most common PRF1 variation in that population with FHL2 (1). Similarly, the variant contrasts with that reported in Turkish patients, with c.1122G>A (p.W374X) being the most prevalent, as in Japan, where the most common was the c.1090-1091delCT variant [22]. The hotspot variation in Chinese FHL2 is in the conserved region 2 of protein kinase C, whereas the one reported here was one at the protein level produces the missense change of an alanine to valine at codon 91 (p.Ala91Val), an amino acid residue located in the functional domain "PERF_HUMAN domain 'MACPF" [21].
Once the pathogenic variant that causes FHL2 has been identified, it is possible to talk about prognosis, perform a complete genetic counseling, implement and initiate targeted treatments that reduce the morbidity and mortality associated with this pathology, due to the fact that current studies have molecules that can change the natural history of the disease and intervene in it.
CONCLUSION
FHL is a disease that presents with an excessive inflammatory syndrome caused by activated T lymphocytes and histiocytosis, which presents with autosomal or recessive chromosome-linked inheritance. In Colombia, there is still no consolidated population burden and it is not part of the recognized orphan diseases [5].
FHL can be divided into five subtypes according to the causative genetic variant. Variants involving PRF1 and UNC13D are the most pathogenic [7]. Worldwide, 58% of FHL patients have variants of the PRF1 gene [4]. Pathophysiologically, the main underlying defect was identified to be altered T cell and NK cell cytotoxicity [1]. Patients carrying defects in the PRF1 gene are vulnerable to infections, autoimmune diseases and malignancies [12]. The main clinical features are persistent fever, hepatosplenomegaly, pancytopenia and decreased NK cell activity [9,10]. To make the diagnosis, the HLH probability calculator (HScore) is in use, which takes into account 9 criteria, with a sensitivity of 93% and a specificity of 86% [13]. As a confirmatory method, the use of a multigene panel or genomic tests are included. The former, includes the analysis of genes involved in known FHL types, such as PRF1, UNC13D, STX11 and UNC18B [17].
Clinical trials are currently underway worldwide on the efficacy and safety of emapalumab as a treatment for patients with HLH, with particular emphasis on long-term outcome and quality of life assessments, some have shown promising results as a controller of disease progression [19,23]. However, this is a rapidly progressive disorder with a high mortality rate if left untreated and the only curative treatment currently available is allogeneic hematopoietic stem cell transplantation (HSCT) [3].
Given the advances in diagnostic aids, confirmatory methods and new pharmacological therapies, it is necessary to conduct more studies to better address this disease, increase screening, describe the population burden, raise awareness of the guild of health personnel to consider this pathology as a differential diagnosis to perform a good genetic counseling. Early identification of this disease is a priority through a complete clinical history and physical examination, knowing the family genetic risks, the importance of population screening and phenotype-genotype correlation in order to be able to talk about perspective, prognosis, follow-up and genetic counseling. With a defined and precise diagnosis, it is also possible to implement and initiate targeted treatments that reduce the morbidity and mortality associated with this pathology, bringing us closer to precision, anticipatory, preventive, predictive and participatory medicine.
ACKNOWLEDGMENTS
To the Universidad Libre seccional Cali, the GRINPED group and the NEUROMET line.
AUTHORS' CONTRIBUTION
JMSV - information search, topic review, writing, editing, submission.
LJMG - writing, editing and final revision of the manuscript.